The Vanderbilt-Ingram Cancer Center (VICC) at Franklin has added new technology to enhance treatment for patients needing radiation therapy or stereotactic body radiation.
The newly installed TrueBeam linear accelerator provides more accurate targeting of the radiation beam to focus on the cancer or lesion and enhanced protection for the adjacent tissue. VICC at Franklin is the first radiation oncology center in the region to use the new TrueBeam technology.
Anthony Cmelak, M.D., professor of Radiation Oncology and medical director of VICC at Franklin, said the new system is faster and safer than previous technologies.
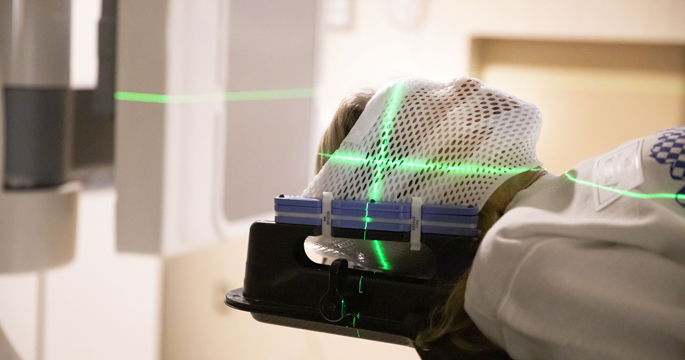
“Historically, the way we have aligned treatments are with lasers to marks on the patient’s skin, we then leave the room and deliver the treatment. This machine can ensure proper patient positioning after we have left the room using “portal imaging” before we turn on the machine,” Cmelak said. “We can then essentially look down the barrel of the beam using either traditional megavoltage X-rays, or new kilovoltage technology provided by the new system. This enables more detailed imaging using a much smaller radiation dose to the patient.”
Linear accelerators feature a series of lead panels or “leaves” that move in and out at pre-set times and angles to help shape the radiation beam. The TrueBeam “leaves” feature an improved design that results in less incidental radiation exposure for the patient.
“The TrueBeam also has the ability to dynamically move its aperture blocking jaws immediately to the edge of the leaves while the beam is treating the patient, which minimizes the leakage between the leaves. This decreases radiation dose to uninvolved organs and tissue,” Cmelak said.
Speed is another feature of the new system, which is 2.5 times faster than the previous linear accelerators in terms of output.
“We can treat patients in far less time and that’s important when we have patients with chronic obstructive pulmonary disease, or claustrophobia, or if we’re treating somebody who doesn’t tolerate lying on a table too long like children or the elderly,” said Cmelak.
The new treatment table offers six degrees of freedom, allowing the operators to leave the room and robotically adjust the height of the table, the foot angle, the in and out position, plus roll, pitch and yaw.
Operators can therefore optimally position the patient for targeting of the radiation beam. The TrueBeam also can image a patient with cone-beam CT once the patient is felt to be in the proper position. This allows visualizing soft tissues of both tumor and adjacent anatomy, which may change day to day as a tumor shrinks, swells, or changes shape. This can be done weekly or even daily to allow true “adaptive radiotherapy.”
The technology also has the capability of doing stereotactic body radiation so clinicians can give larger doses in fewer fractions which is ideal for treating issues like lung cancer or spine lesions.
Cmelak said the targeted accuracy of the device allows clinicians to safely deliver bigger doses per day.
“That’s especially helpful for some tumors like melanoma and renal cell cancer where we can give bigger doses each day and overcome their inherent radio-resistance,” said Cmelak.
The new technology also has an important feature. Clinicians can set parameters for the machine to turn off and on automatically if a tumor moves in and out of the beam as the patient breathes.
This “gating” feature is just one more example of the improved safety of the new technology.
A second TrueBeam system is expected to be installed on the main campus at VICC later in the year.